The Australian Government’s $7.9 billion investment in Medicare, set to take effect on November 1, 2025, represents the most significant policy shift for general practice in a generation. This landmark reform introduces a dual-pronged approach to revitalise bulk billing: a universal expansion of existing incentives and a new, voluntary program designed to reshape the financial landscape for practices willing to commit to a fully bulk-billed model. This new framework places every general practice in the country at a pivotal strategic crossroads. In this blog we’ll break down the numbers to help practices understand the mechanics of the new incentives, model the financial impact, navigate the operational requirements, and make an informed decision that aligns with their business objectives and practice philosophy.
Recap: The two main components of the increased bulk billing incentives
Part 1: Universal expansion of standard bulk billing incentives
This is a foundational change with practice-wide implications. From November 1, 2025, eligibility for the existing Medicare Benefits Schedule (MBS) bulk billing incentive payments will be expanded. Previously, these incentives were restricted to services provided to children under 16 years of age and Commonwealth concession card holders. The reform extends eligibility to all Medicare-eligible Australians.
This means that for any patient a practice chooses to bulk bill, even within a mixed-billing model, an additional incentive payment can be claimed on top of the standard MBS rebate. This change provides a baseline revenue uplift for all practices, regardless of their participation in the new practice-level program, for any services they are already bulk billing for non-concession patients.
Part 2: The Bulk Billing Practice Incentive Program
Layered on top of the universal bulk billing incentive expansion is the new Bulk Billing Practice Incentive Program (BBPIP), a voluntary program designed to encourage practices to adopt a 100% bulk-billing model for eligible services. The government’s stated objective is to triple the number of fully bulk-billed practices nationally to approximately 4,800. Participation in the BBPIP is entirely optional, and practices can choose to opt-in or opt-out at any time, providing a degree of flexibility. This structure creates a clear choice: practices can leverage the universal BBI uplift within their existing billing model and additionally choose to commit fully to the BBPIP to access an additional, though more restrictive, incentive.
Amazing, we are all back up to speed on what’s coming from November 1st, now onto the new stuff.
The BBPIP: The 12.5% Loading and the new 50/50 Split
Announced on the 15th of August, the 12.5% practice incentive provided to practices that sign up to universal bulk billing will be shared equally between participating practices and practitioners.
How the incentive is calculated
Practices participating in the BBPIP will receive an additional quarterly incentive payment. This payment is calculated as 12.5% of the total MBS benefits earned from all eligible services provided during the previous quarter. This 12.5% “loading” is paid in addition to both the standard MBS benefit and the universal Bulk Billing Incentive (BBI) claimed for each individual service.
Which services are eligible?
The full list of eligible services can be found via the Department of Health here.
The Mandated 50/50 Split
Following consultations with the medical sector, the government has confirmed that this 12.5% bulk billing incentive payment (new BBPIP) will be split evenly, 50/50, between the General Practitioner who provided the service and the practice itself. This legislated split is intended to formally acknowledge the distinct contributions of both the individual clinician and the practice’s infrastructure in the delivery of bulk-billed care.
This mandated split has the potential to add additional layers of complexity in the typical financial relationship between GPs and practices. For many clinics operating on a service fee model where the GP pays a percentage of their total billings (e.g., 30%) to the practice, this new, fixed 50/50 distribution for the BBPIP revenue stream may conflict with existing practitioner agreements. Practices will need to proactively review and assess how this specific payment is handled, ensuring financial transparency and preventing future disputes.
Systems like Cubiko Calculate can also be used to implement a variety of service fee rules in order to implement more complex contractual agreements, which reflect the increasing complexities of our primary care industry.
Accessing the BBPIP
The administration of the BBPIP is designed to be automated. Services Australia will assess a practice’s claiming data at the end of each quarter to verify compliance. Payments will be made in arrears, with the first payments for the November-December 2025 period scheduled for the first quarter of 2026. The funds will be distributed directly to the nominated bank accounts listed in the MyMedicare Organisation Register for the practice and in the individual GP’s Health Professional Online Services (HPOS) account.
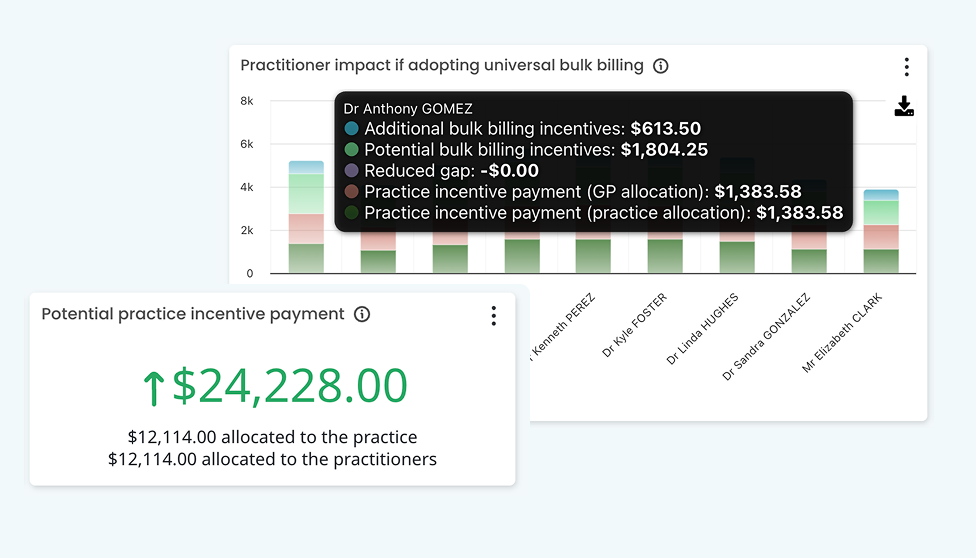
Where to find your practice’s potential bulk billing incentive figures
We’re pleased to share that Cubiko has just released updates to its potential bulk billing incentives metrics, now including and reflecting the 50/50 split of the PIP between the practice and practitioner. Using Cubiko Insights you can gain a simple look into how each individual practitioner may benefit from the new incentives as well as what these incentives could look like for practice revenue. If you aren’t already using Cubiko Insights, book a demo with the team to learn more!